
 Australia; VIC; QLD; SA
Australia; VIC; QLD; SA
News release
From:
An international team has analysed over 2,000 people’s behaviours within a 24-hour day to determine the optimal amount of time we should spend sitting, sleeping, standing and being physically active within a 24-hour period for optimal health.
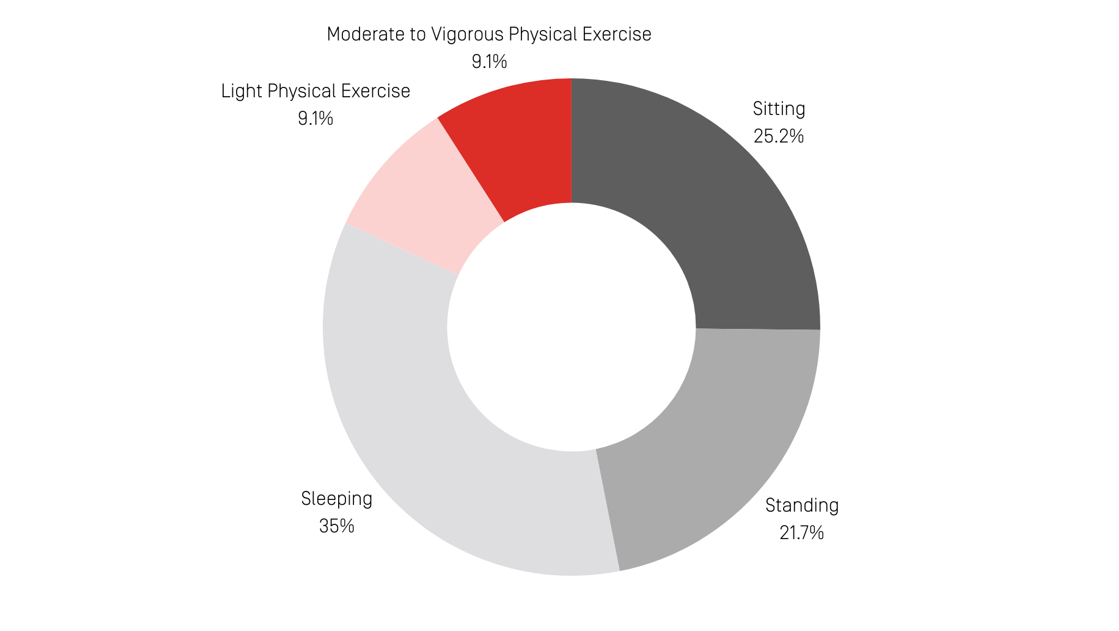
According to the new research from Swinburne University of Technology and the Baker Heart and Diabetes Institute, the ideal daily balance is associated with:
- Six hours of sitting
- Five hours and 10 minutes of standing
- Eight hours and 20 minutes of sleeping
- Two hours and 10 minutes of light-intensity physical activity
- Two hours and 10 minutes of moderate-to-vigorous intensity physical activity
While light-intensity physical activity could range from chores to making dinner, moderate-to-vigorous physical activity involves more intentional movement such as a brisk walk or gym workout.
Dr Christian Brakenridge from Swinburne’s Centre for Urban Transitions led the international team and says that these measures are a ‘goldilocks zone’ that strikes a balance between various health outcomes.
“For different health markers, from waist circumference to fasting glucose, there would be different levels for each behaviour. This breakdown encompasses a wide range of health markers and converges on the 24 hours associated with overall optimal health.”
For example, the research findings suggest that replacing time spent sitting with greater time in physical activity, especially light-intensity physical activity, was associated with more beneficial blood glucose measures in those with type 2 diabetes than those without.
Dr Brakenridge says that his research could be used by the Federal Government when they release their new activity guidelines, which currently only include wide parameters around exercise and intensity.
While many guidelines do not consider how different behaviours overlaps and interact, Dr Brakenridge’s research acknowledges the nuances of how one activity impacts the rest of the day.
“Sleeping may be detrimental to health if it replaces exercise time, but beneficial if it replaces sedentary behaviour. This is why we need integrated guidelines considering the full spectrum of human behaviour,” he says.
“People may advocate for more time exercising, though it’s not feasible to have 10 hours of exercise and zero hours of sedentary behaviour – the time use has to be realistic and balanced.”
“Of course, moving as much as you can is always encouraged when so much of life requires us to be sitting in front of screens. Shorter sitting time and more time spent standing, undergoing physical activity and sleeping give great boosts to our cardiometabolic health.”
“It’s also important to acknowledge that this data is a recommendation for an able adult. We all have different considerations, and above all, movement should be fun.”

