
 Australia; International; NSW; VIC
Australia; International; NSW; VIC
News release
From:
Decades-old theory debunked to explain rare immune condition
Australian researchers have discovered that key immune cells malfunction in a potentially life-threatening disease, pointing to new treatment possibilities with existing drugs.
Researchers at the Garvan Institute of Medical Research have uncovered a critical mechanism driving inflammation in mevalonate kinase deficiency (MKD), a rare but devastating autoinflammatory disorder. The study, published today in Immunity, reveals that immune cells called natural killer (NK) cells are impaired in MKD, leading to an excessive inflammatory response when patients encounter infections.
The findings challenge 30 years of scientific assumptions about the disease and suggest that medications called JAK inhibitors could provide relief for patients when other drugs don’t work.
“This study has revealed a new target for this inflammatory disorder and sets the scene for future clinical studies to explore the use of JAK inhibitors or other drugs to neutralise interferon gamma in patients with MKD,” says Professor Mike Rogers, Lab Head at Garvan and senior author of the study. “This could lead to a targeted treatment that hasn’t been tried before.”
The mechanics of a misfiring immune system
MKD is a lifelong disease affecting hundreds of children and adults worldwide, though experts believe many more cases go undiagnosed. People with the condition experience frequent episodes of high fever, skin rashes, joint pain and abdominal inflammation. In severe cases these inflammatory flares can be life-threatening.
For decades, scientists believed immune cells called macrophages were responsible for inflammation in MKD. Current treatments target an inflammatory signal produced by macrophages, but these therapies fail in about half of all patients, leaving many without effective care.
To find out why, the Garvan research team used preclinical models of MKD and patients’ blood samples to investigate what goes wrong in the immune system. They discovered that different immune cells called NK cells – the body’s first line of defence against viral infections – cannot mature and don’t work properly at fighting infection.
This failure of NK cells to work properly triggers a domino effect that causes inflammation.
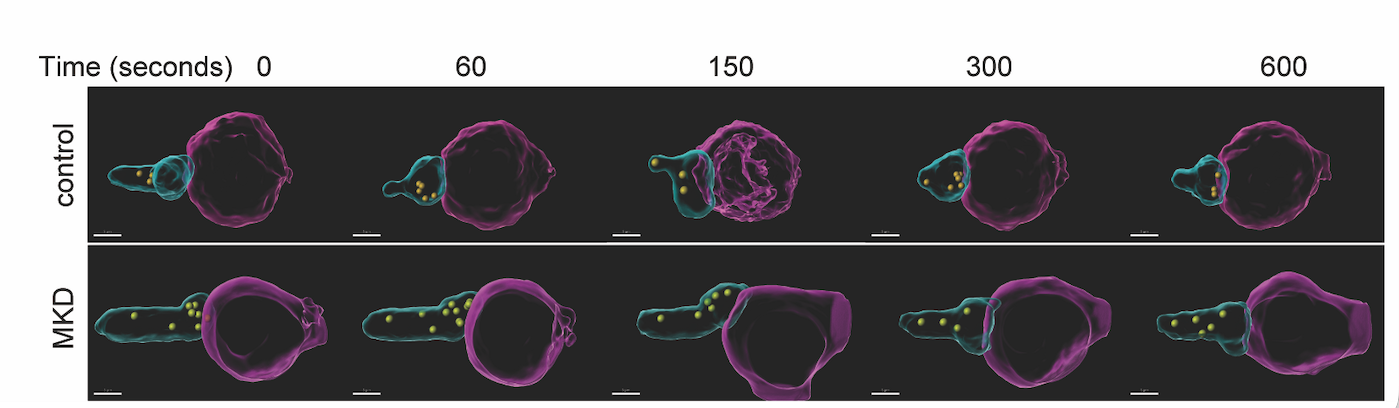
“We found that these immune cells are essentially misfiring,” explains Professor Rogers. “NK cells are loaded with toxic ammunition, stored in granules that are released to kill infected cells. However, in MKD these toxic granules can’t be released from NK cells and remain trapped inside. When an NK cell fails to kill its target, it compensates by shouting for help, pumping out large amounts of interferon gamma – a powerful inflammatory signal. This activates other immune cells and causes the dangerous fever and widespread inflammation seen in patients.”
Challenging established thinking about the disease
Lead researcher Dr Marcia Munoz, Group Leader in the Rogers Lab, says the study is a fundamental shift in our understanding of MKD.
“This really turns on its head 30 years of dogma about what was thought to be the underlying mechanism of disease. In MKD, the primary problem is in NK cells and not in macrophages, as previously believed,” she says.
Working in collaboration with Professor Mariapia Degli-Esposti and researchers at Monash University, the team used preclinical models to confirm the link between the dysfunction in NK cells and patient symptoms. They demonstrated that the inability to clear a viral infection leads to the severe inflammatory organ damage seen in MKD.
New treatment approach shows promise
Based on their findings, the researchers worked with clinicians at the Royal Children’s Hospital in Melbourne to treat an infant with severe MKD using baricitinib, a JAK inhibitor that blocks interferon signalling. The medication is already used to treat other immune disorders such as rheumatoid arthritis and eczema.
When baricitinib was added to the infant’s standard therapy, clinicians observed a reduction in disease severity – including fewer flares and healing of severe gastrointestinal inflammation – demonstrating the potential of this new approach.
Implications for related disorders
For the family of genetic diseases that affect the same metabolic pathway as MKD, the researchers have coined the term ‘prenylopathies’. Their preliminary work suggests these related conditions may be driven by the same issue: NK cells malfunctioning and misfiring.
“Confirming this link could help end the diagnostic odyssey many patients endure for years or even decades before receiving effective treatment,” says Professor Rogers.
Professor Mike Rogers is a Conjoint Professor at St Vincent's Clinical School, Faculty of Medicine and Health, UNSW Sydney. Dr Marcia Munoz is a Conjoint Senior Lecturer at St Vincent's Clinical School, Faculty of Medicine and Health, UNSW Sydney.
Multimedia


Attachments
Note: Not all attachments are visible to the general public. Research URLs will go live after the embargo ends.


